What ADHD Looks Like in Childhood
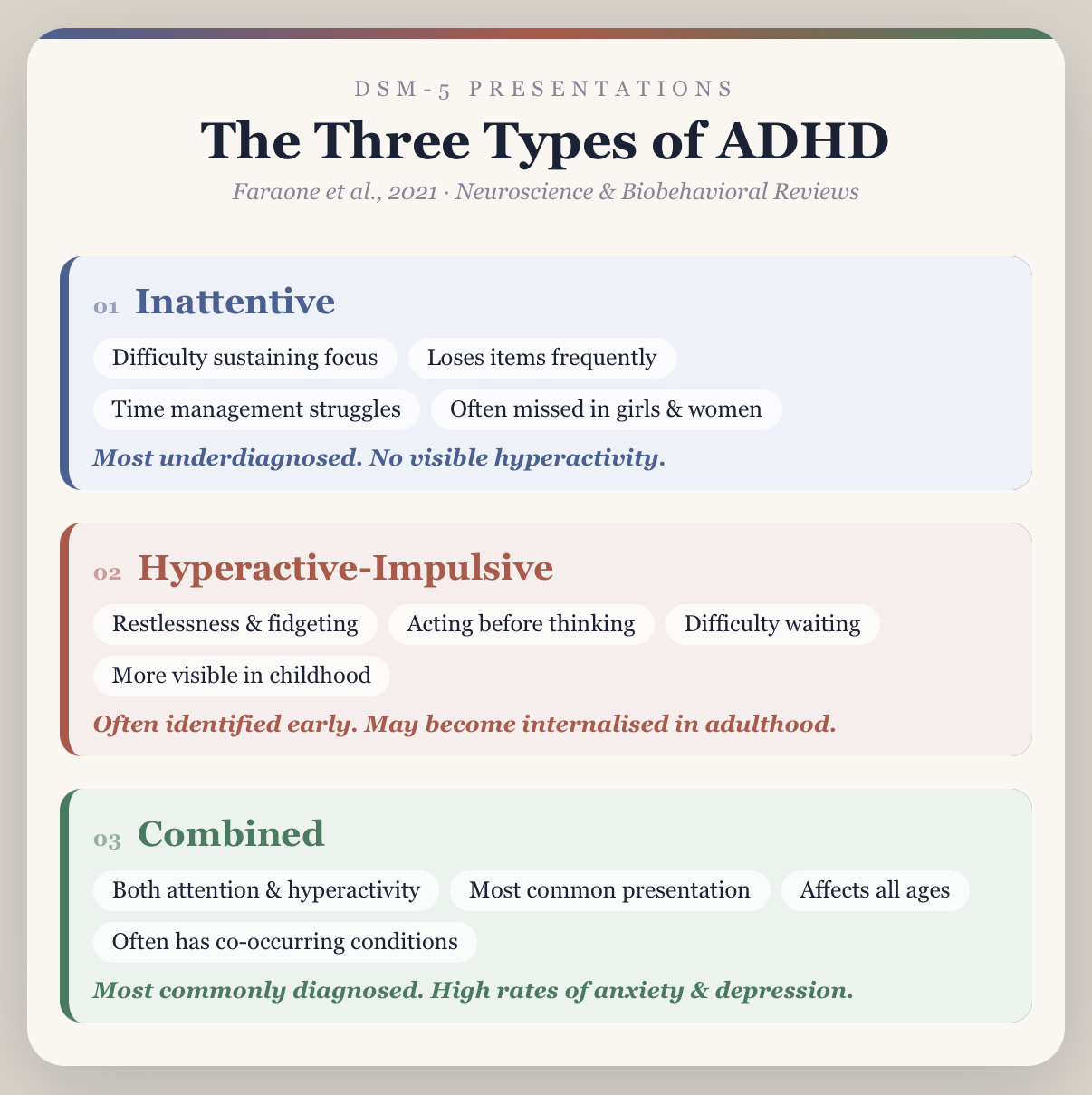
ADHD in childhood is more visible than in adulthood, but the picture most parents and teachers carry is still incomplete. The child who cannot sit still, calls out answers before others have finished, and struggles to remain in their seat represents only one presentation. The child who sits quietly at the back of the classroom, drifts through lessons without complaint, and never quite finishes the task in front of them may equally have ADHD, and is far less likely to be noticed, referred, or supported.
In primary school-aged children, ADHD most commonly presents as difficulty sustaining attention on structured tasks, persistent disorganisation across home and school, impulsivity in social situations, and an inability to regulate activity level when the environment requires stillness and compliance. What the classroom sees as inattention or behaviour is frequently a child working at the edge of their regulatory capacity in an environment that makes few accommodations for how their brain actually functions.
A significant and often underappreciated feature of childhood ADHD is the early impact on emotional experience. Children with ADHD are more likely to experience intense frustration, low tolerance for perceived failure, and difficulty in peer relationships - not because of temperament, but because emotion regulation is itself a core executive function affected by the condition [1]. Rejection sensitivity and social difficulties emerge early and, without support, tend to compound over time.
ADHD also presents differently across developmental stages. In preschool-aged children, hyperactivity and impulsivity are most prominent. In primary school years, the demands of sustained seated attention and structured work bring inattentive difficulties into sharper relief. In adolescence, external hyperactivity often reduces while internal restlessness, academic underperformance, and emotional dysregulation become more prominent. Girls are significantly more likely to present with inattentive symptoms throughout childhood, are less likely to be referred, and on average receive a diagnosis several years later than boys with equivalent difficulties [4]. Co-occurring anxiety, behavioural difficulties, and sleep problems are common in children with ADHD and are frequently treated in isolation unless a comprehensive assessment identifies the underlying neurodevelopmental picture [1].
What ADHD Looks Like in Adulthood
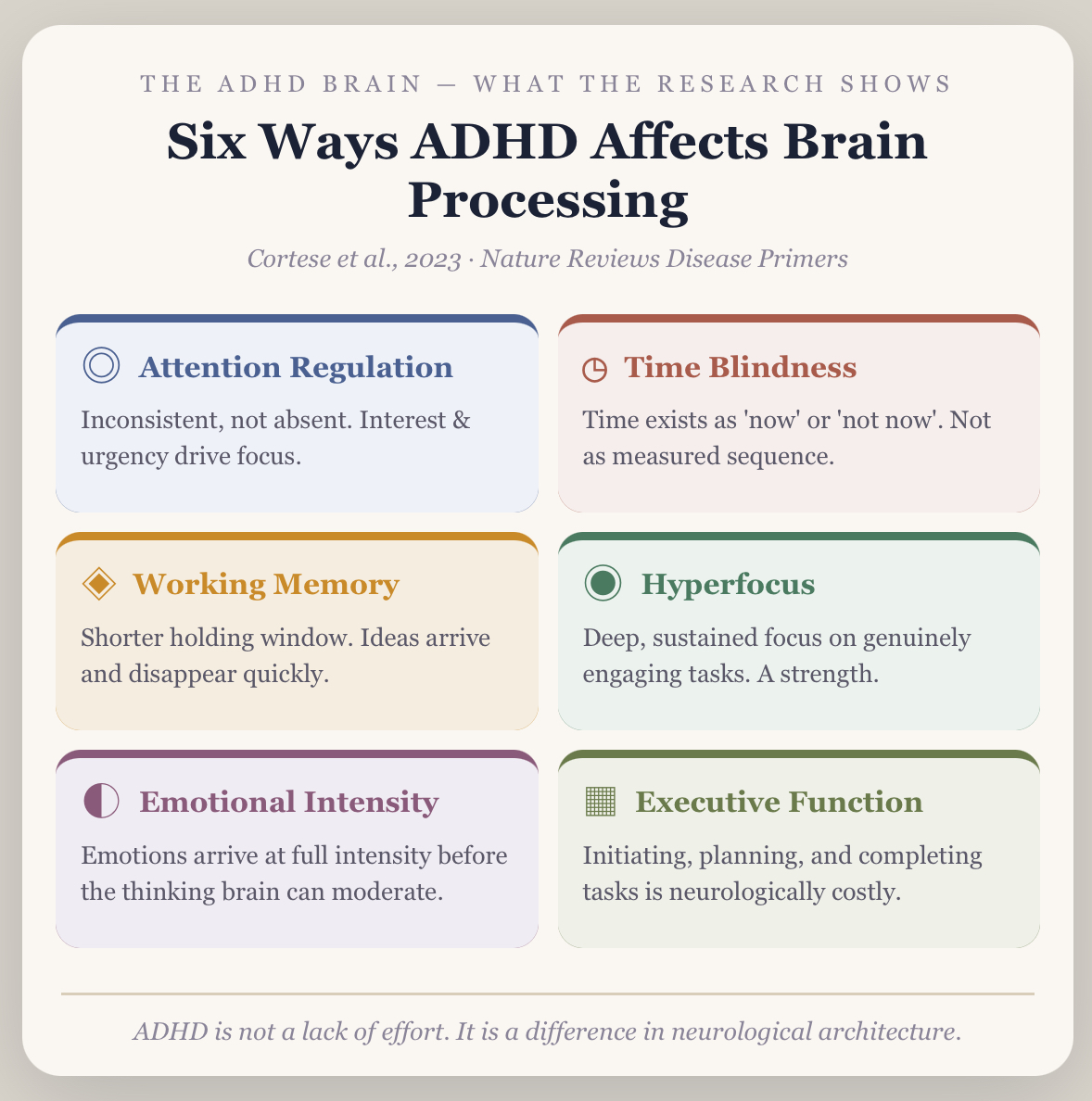
Adult ADHD looks different from the classroom picture most people carry. Hyperactivity is often internalised as racing thoughts, an inability to settle, and chronic restlessness rather than physical movement. The more visible presentations are difficulty meeting deadlines despite genuine effort, time blindness (a neurological difficulty perceiving the passage of time accurately), chronic procrastination on high-priority tasks, and underperformance relative to measured intellectual ability.
A significant and often overlooked feature of adult ADHD is emotional dysregulation. Research published in leading psychiatric journals has established that difficulty managing emotional intensity is not simply a comorbidity of ADHD for many people, it is a core feature [2]. This manifests as intense frustration, rapid mood shifts, rejection sensitivity, and a disproportionate emotional response to situations that others find manageable.
Co-occurring conditions are common and are frequently misidentified as the primary diagnosis. Anxiety, depression, sleep problems, and stress are all significantly more prevalent in individuals with ADHD than in the general population, and often develop as secondary consequences of years of unmanaged ADHD rather than as independent conditions [1].
The Cost of a Missed Diagnosis in Childhood
The consequences of unidentified ADHD in childhood are not confined to the classroom. Children who move through their school years without assessment or support do not simply fall behind academically. They accumulate something harder to measure: a story about themselves. Each year of unexplained difficulty, each teacher report about potential not being met, each moment of watching peers manage what feels impossibly hard, contributes to a self-concept built on the assumption that the problem is personal rather than neurological.
The practical costs are significant. Children with undiagnosed ADHD are more likely to experience academic underperformance relative to measured ability, social difficulties and peer rejection, family conflict arising from behaviour that parents have been told should be within the child's control, and school refusal when the gap between expectation and capacity becomes unmanageable [1]. Without early identification, the developmental window for establishing effective strategies, school-based accommodations, and family approaches narrows considerably.
A diagnosis in childhood does not eliminate difficulty. What it changes is the framework available to the child, their family, and their teachers. It replaces a narrative of effort and attitude with an accurate clinical explanation, and opens access to targeted interventions, NDIS support where applicable, and individual therapy genuinely adapted to how the child's brain works. Research consistently demonstrates that early identification and intervention improves long-term educational, social, and emotional outcomes for children with ADHD [1].
The Cost of a Missed Diagnosis in Adulthood
The consequences of unidentified ADHD across a lifetime are not trivial. Adults who reach assessment without a prior diagnosis have typically spent years developing compensatory strategies, elaborate systems, excessive lists, and reliance on external deadlines that work until they do not. Career disruption, relationship difficulties, financial disorganisation, and a persistent and painful gap between potential and performance are common presentations in adults seeking assessment for the first time.
A diagnosis in adulthood does not change the past. What it does change is the framework through which the past is understood, and the range of targeted evidence-based interventions that become available once the correct clinical picture is established [5].



.webp)
